Foram encontradas 90 questões.
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
The excerpt that contains a comparison is:
Provas
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
“Nor” in “nor can it be explained” (1st paragraph) signals a(n)
Provas
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
The last sentence carries a
Provas
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
According to the text, some offenders may get away with punishment because of their
Provas
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
Based on the text, mark the statements below as true (T) or false (F).
( ) Gender inequity in medical leadership is due to few women who want to take leading positions.
( ) Difference between genders has little effect when disciplining transgressive attitudes at work.
( ) Women physicians have been found to improve the quality of health care services.
The statements are, respectively,
Provas
A figura a seguir ilustra uma pirâmide de base pentagonal.
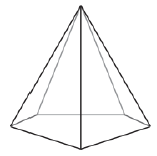
Duas dessas pirâmides idênticas foram coladas pelas bases formando um novo sólido com 7 vértices e 10 faces.
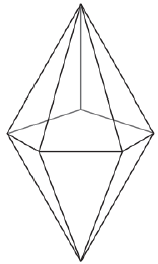
Nas proximidades de cada um desses 7 vértices, são feitos cortes no sólido produzindo 7 pequenas pirâmides que serão, posteriormente, removidas. A esse processo se chama truncamento.
Após o truncamento descrito, o sólido passará a ter
Provas
A figura a seguir ilustra uma parede retangular de 6,0 m de largura e 3,0 m de altura.
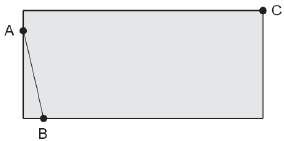
Um cabo de energia elétrica retilíneo liga duas tomadas localizadas nos pontos A e B, estando A sobre a borda esquerda da parede, a 50 cm da borda superior. O ponto B está na base da parede, a 50 cm da sua borda esquerda.
Deseja-se passar um outro cabo retilíneo que ligue o ponto C, na quina da parede, a um ponto D na mesma borda que contém o ponto A. Sendo esse um cabo de internet, é fundamental que passe pelo cabo AB perpendicularmente.
Uma das formas de se determinar a posição do ponto D é imaginar eixos cartesianos !$ vec{Ox} !$e !$ vec{Oy} !$ colocados, respectivamente, sobre as bordas inferior e esquerda e tratar os cabos como segmentos de retas perpendiculares.
A distância do ponto D à base inferior da parede é igual a
Provas
Uma confecção produz calças jeans e conclui que a quantidade !$ Q !$ de unidades vendidas mensalmente depende do preço !$ p !$ cobrado por unidade conforme a função !$ Q(p)=200-p !$.
O custo de produção mensal dessas calças é composto por um valor fixo de R$ 400 acrescido de R$ 25 por unidade produzida, ou seja:
!$ C(p) = 400 + 25 cdot Q(p) !$
Para calcular o valor !$ A !$ arrecadado no mês com as vendas, multiplica-se o preço unitário !$ p !$ pela quantidade !$ Q !$ de unidades vendidas no período.
O lucro mensal !$ L !$ apurado no mês é dado pela diferença entre a arrecadação !$ A !$ e o custo !$ C !$.
Em um mês em que forem vendidas 150 unidades, o lucro será de
Provas
A quantidade de trios diferentes que podem ser feitos escolhendo-se 3 pessoas em 6 disponíveis é 20. Para encontrar esse valor, primeiro utiliza-se o Princípio Fundamental da Contagem (6!$ imes !$5!$ imes !$4). Em seguida, divide-se o resultado por !$ 3! = 6 !$ para corrigir o erro de repetição de contagem de agrupamentos repetidos como !$ ABC !$, !$ ACB !$, !$ BAC !$, !$ BCA !$, !$ CAB !$ e !$ CBA !$.
Entretanto, se houver alguma característica que distinga uma delas das outras 2, a correção deve ser feita dividindo-se 6!$ imes !$5!$ imes !$4 por 2!.
Com base nessas informações, pode-se concluir que, dadas 8 pessoas, a quantidade de diferentes grupos formados por 4 indivíduos, em que uma delas é chefe do grupo e que alguma outra seja porta-voz do grupo é
Provas
Um sinalizador !$ P !$ é disparado para o alto e, ao atingir 8!$ pi !$ metros de altura, começa a cair em trajetória helicoidal. A figura a seguir ilustra o percurso feito pelo sinalizador sobre um sistema cartesiano do !$ mathbb{R}^3 !$.
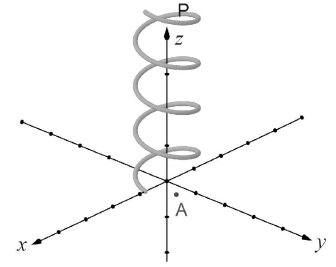
Nesse sistema, a posição do ponto !$ P !$, em função do tempo !$ t !$ (em segundos), é dada pelas coordenadas
!$ x=4cdot cos(t)\y=4cdot sen(t) \ z = 8pi - t !$
estando !$ x !$, !$ y !$ e !$ z !$ em metros. O plano !$ xOy !$ é o piso horizontal onde o sinalizador encerrará sua queda e !$ A !$ é a projeção ortogonal de !$ P !$ nesse mesmo plano a cada instante.
Durante a queda, na última vez em que as coordenadas de !$ A !$ forem (2!$ sqrt{3} !$;2), a altura do sinalizador !$ p !$, em relação ao solo, será
Provas
Caderno Container